


INTRODUCTION
It is usually reported that clear cell renal cell carcinoma (ccRCC) has been implicated as a cause of trapped lung through the development of malignant pleural effusion1. Endobronchial metastases due to renal cell carcinoma are rare2. There is only one case report that these metastases cause complete atelectasis of the left lung2.
Here, we present a rare case of a 63-year-old male who presented with a right massive pleural effusion as a result of metastatic renal cell carcinoma, which caused a right trapped lung, due to endobronchial obstruction.
CASE REPORT
A 63-year-old patient, ex-smoker (80 pack-years), with a known history of metastatic clear cell renal cell carcinoma (ccRCC) under chemotherapy, with brain, endobronchial and liver metastases (Performance status: 3), chronic obstructive pulmonary disease (COPD), atrial fibrillation and arterial hypertension, presented to the Emergency Department (ED) complaining of shortness of breath on exertion (mMRC: 4/4) only in the left lateral recumbent position. The patient was bronchoscoped 8 months ago due to a lesion in the right lung. Bronchoscopy had revealed partial obstruction <50% in the right main lung, where biopsies had been taken from the lesion. Physical examination showed peripheral edema in both legs and auscultation revealed decreased breath sounds and decreased tactile and vocal in the right lung. In the ED, a chest X-ray showed increased density of the right hemithorax. Laboratory testing revealed elevated serum C-reactive protein (CRP), whose value was 131 mg/dL, and normochromic normocytic anemia with Hb levels at 8.1 g/dL, MCV at 90.2 fL, MCH at 29.5 pg. The differential diagnosis was based on the above in hemothorax and malignant pleural effusion. Subsequently, a chest Computed Tomography (CT) showed a right hilum lung mass extending to the right main bronchus causing complete atelectasis of the affected lung and a large pleural effusion (Figure 1).
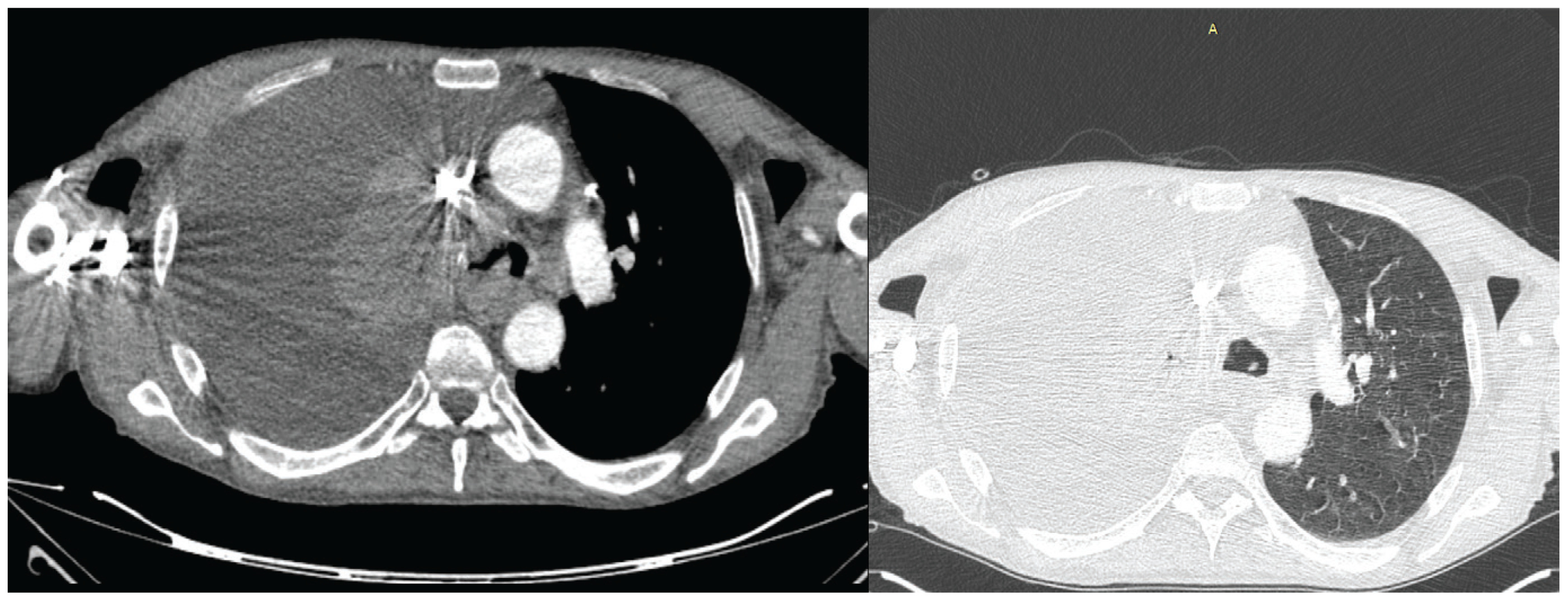
Figure 1
The chest computed tomography (CT) showed a right hilum lung mass extending to the right main bronchus causing complete atelectasis of the affected lung and a large pleural effusion
The patient was treated with oxygen therapy with a nasal cannula at 2 L/min.
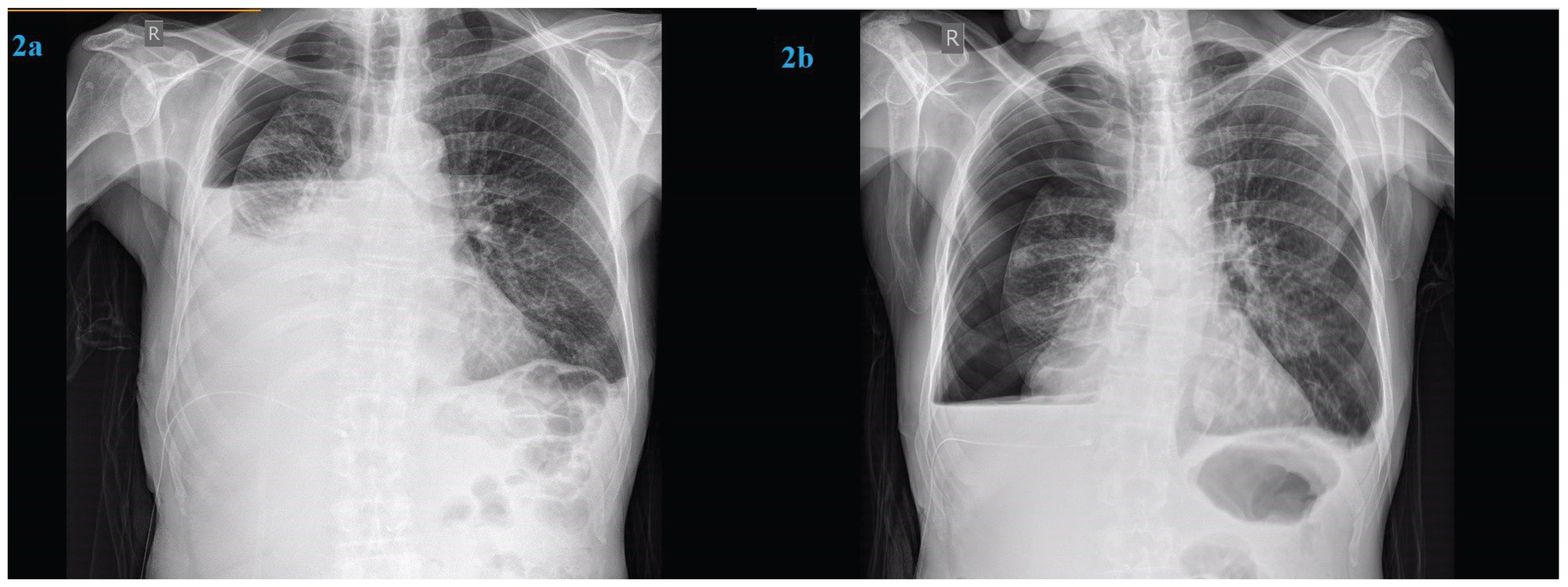
However, as soon as the patient was placed in the left lateral recumbent position to insert a small-bore chest tube (14F) into the pleural cavity, he felt severe dyspnea, resulting in increasing oxygen requirement. The chest tube was successfully inserted and the patient was placed on the supine position again with clear easing of dyspnea and gradually as oxygen requirements decreased, supplemental oxygen was titrated downwards. About 1500 mL of fluid, which was a transudate, was removed. Post-drainage chest X-ray, 24 hours later, revealed a hydropneumothorax suspicious for a pneumothorax ex-vacuo (trapped lung) as shown in Figure 2a. The chest tube was placed on suction without any additional re-expansion of the lung (Figure 2b). Two days after the chest tube placement, the patient passed away, before undergoing bronchoscopy, in which electrocoagulation would be used.
DISCUSSION
Endobronchial metastases are rare; however, it has been observed that 80% of these cases involve the right lung3. This finding is unclear up to today. The condition known as a ‘trapped lung’ is when the lung is unable to expand normally in the thoracic cavity and a residual cavity is seen between the two layers of pleura1,4. Renal carcinomas are among the 3 most common intrabronchial metastases1.
Most patients with trapped lungs are asymptomatic or have minimal dyspnea on exertion1, due to ventilation-perfusion mismatch within the entrapped lung4. It is known that in patients with pulmonary diseases, dyspnea occurs when they lie on the lateral side with the affected lung down5,6.
Our patient experienced dyspnea in the left lateral decubitus position due to elevated pleural fluid levels and cardiac compression on the healthy lung, resulting in atelectasis and trepopnea. An additional potential mechanism is the deterioration of diastolic function while in the left lateral decubitus position7.
Reviewing the literature on the treatment of trapped lung, it is observed that the treatment is aimed at symptomatic management of dyspnoea1,4. This is accomplished by draining the effusion either by minimally invasive techniques or surgically1,4. This is because the management of trapped lungs from pleural causes of non-expandable lungs has been mainly studied1,4.
In our patient this approach did not treat the cause of the trapped lung, nor did it relieve the symptoms of dyspnea.
For patients with advanced-stage endobronchial metastasis palliative therapy is available, including transthermal traps, forceps capture under a rigid bronchoscope, intrabronchial radiation (brachytherapy), photodynamic therapy, electro-coagulation, prosthetic stents, intrathoracic ethanol injections, and Nd:Yag laser ablation therapy. These treatments are intended to enhance the quality of life rather than to heal the patient and are performed in big experienced centers with these techniques. Pneumonectomy and lobectomy are also indicated in patients with limited endobronchial metastatic lesions8.
CONCLUSION
We reported a rare case of endobronchial metastasis due to clear cell renal cell carcinoma (ccRCC) that caused a right trapped lung, after reviewing the existing literature. This case illustrates the complex approach and alternative treatment modalities that a pulmonologist should consider when presented with the totality of the case data, as the first step in the management of a massive pleural effusion is the placement of pleura catheter to decompress the patient and improve the patient’s sense of dyspnea. We hope to draw more attention to this underdiagnosed entity, so that there is early management with endobronchial techniques.