


INTRODUCTION
The tobacco epidemic is one of the most significant public health warnings in the world according to the World Health Organization; 8 million people die each year due to smoking, 7 million of them die due to direct smoking, and 1.2 million are not tobacco users and lose their lives due to exposure to secondhand smoke1. Today, hookah is known as a traditional smoking method2. hookah is known by different names such as hookah, narghile, argileh, shisha, goza boory, hubble bubble etc., which have different shapes and sizes according to the place and type of tobacco. Still, the common feature of all of them is the passage of smoke through water before inhalation by the consumer3. The results of a survey on tobacco use showed that hookah smoking in the last 12 months in students in grade 12 in the United States increased from 17.1% per 6 students in 2010 to 22.9% per 4 students in 20144. This global study in 7 Middle Eastern countries also showed that hookah smoking in all countries studied in the Middle East is higher than smoking5.
Many studies show a link between hookah smoking and many problems, including cancer, infectious diseases, and chronic diseases6,7. Akl et al.6, in their study, showed that in the minds of people, the dangers of the smoking hookah are less than smoking, and smoking hookah is more socially acceptable than smoking. However, the blood nicotine level of people who smoke hookah is similar to that of people who smoke 10 cigarettes a day8.
In a study among young people, the highest prevalence of hookah smoking in the last 30 days was reported in Lebanon with 36.9%, the West Bank 32.7%, and Eastern Europe (Latvia 22.7%, Czech Republic 22.1%, Estonia 21.9%)9. According to Mumtazi and Rawson10, 34.4% of high school girls in Iran have experienced hookah smoking during their lifetime. In the study of Kassem et al.11, the prevalence of hookah smoking in boys and girls was 25.7%, and 60.6% of boys and 53.1% of girls had experienced hookah smoking during their lifetime11. The study results showed that hookah smokers smoke hookah as an enjoyable entertainment among their friends regardless of the health consequences12. The results show that hookah smoking is addictive. In fact, there is a significant amount of addictive nicotine in tobacco. It has been proven that nicotine levels in the blood plasma of smokers increase after smoking a hookah13. Charcoal used to heat tobacco can also increase health risks by producing large amounts of carbon monoxide, metals, and cancer-causing chemicals14. In one hour of hookah smoking, the volume of smoke entering the lungs is approximately 90 L, significantly more than the smoke from 1 cigarette (about 600 mL)15,16.
In their study in the Eastern Mediterranean region, Afifi et al.12 showed that identifying the determinant factors of hookah smoking and planning future interventions to control it throughout society is essential. Therefore, the present systematic review was conducted to determine the effect of interventions to prevent and reduce hookah smoking among hookah smokers.
METHODS
According to the purpose of the study, keywords related to hookah smoking were selected. Then, the search terms were developed as according to the rules in Supplementary file Table 1. To identify related studies for systematic study, electronic databases were searched. To evaluate the inclusion and exclusion criteria of the study, the PICO index (study population, study type, types of determinants) is used17. The period of published studies from the early establishment of the search databases until 2021, which were performed in interventions to prevent and reduce hookah smoking, were examined.
Screening
First, the databases were examined and searched by one of the researchers using the desired search strategy. Then, all identified articles from different the databases were collected using Endnote software, and duplicates deleted in the Endnote folder. Then, the two researchers independently reviewed all the articles and deleted the articles unrelated to the inclusion criteria. Then, two researchers reviewed the abstracts of the remaining related articles, independently. In the next step, the full text of the remaining articles is reviewed by two researchers to determine the articles that meet the inclusion and exclusion criteria. After the final articles were identified, all their references were reviewed. Also, in all stages, from reading the titles to the final approval of the articles, the disputes were resolved through discussion, and finally with the third party’s opinion.
Inclusion criteria
Articles included were interventional studies, for all age groups, both female and male. The language was either English and Persian, regardless of the time limit.
Exclusion criteria
Articles that were excluded were descriptive, qualitative, review, structured review, meta-analysis studies, and studies in which the prevention and hookah reduction is associated with other interventions to implement healthy behaviors.
Data extraction
The data were extracted so that a summary of the features of the articles was examined and recorded in a designed table that included the following:
Names of authors and year of publication of the study;
Study population, including all age groups, both female and male;
Types of interventions including educational interventions and behavioral interventions; and
Types of consequences where the results were evaluated for the most effective type of intervention regarding the impact on the influential factors associated with hookah smoking.
Study quality check
To determine the quality of the articles, two trained researchers reviewed the articles, and the final articles were recorded in a summary of pre-determined tables after review. They were carefully analyzed based on the general-purpose and sub-objectives. EPHPP, developed by the National corporation Center for Methods and Tools (NCCMT) for a variety of studies, was used to evaluate the quality of the studies. Using this tool, one of the general qualities, including strong, medium, and weak, can be assigned to each article.
The quality assessment using this tool is based on the evaluation of 5 components, which include the following: sample selection bias, study type, confusers, data collection methods, and sample attribution18. The quality of studies based on this tool was done by two researchers separately. Finally, to determine the quality of studies, any disputes between the two people were resolved through discussion. Kappa coefficient was used to examine the agreement between the two reviewers19. Also, no study was excluded due to poor quality.
Article selection
The initial search resulted in 4170 article abstracts (Figure 1). A total of 3850 articles were excluded from the study due to irrelevance. Then, the abstracts of the remaining 320 articles were reviewed, of which 65 articles were eligible for inclusion in the study. The full text of the remaining 65 articles was reviewed independently by two researchers. After reviewing the text of the study, out of 65 articles, 44 articles were removed (4 articles due to being a review article, 3 articles due to biological factors of recurrence, 5 articles due to duplication, 8 articles due to publication of the article in both Persian and English, 23 articles due to unrelated topic, 1 article due to being a dissertation. Finally, 21 studies were identified for evaluation (Table 1).
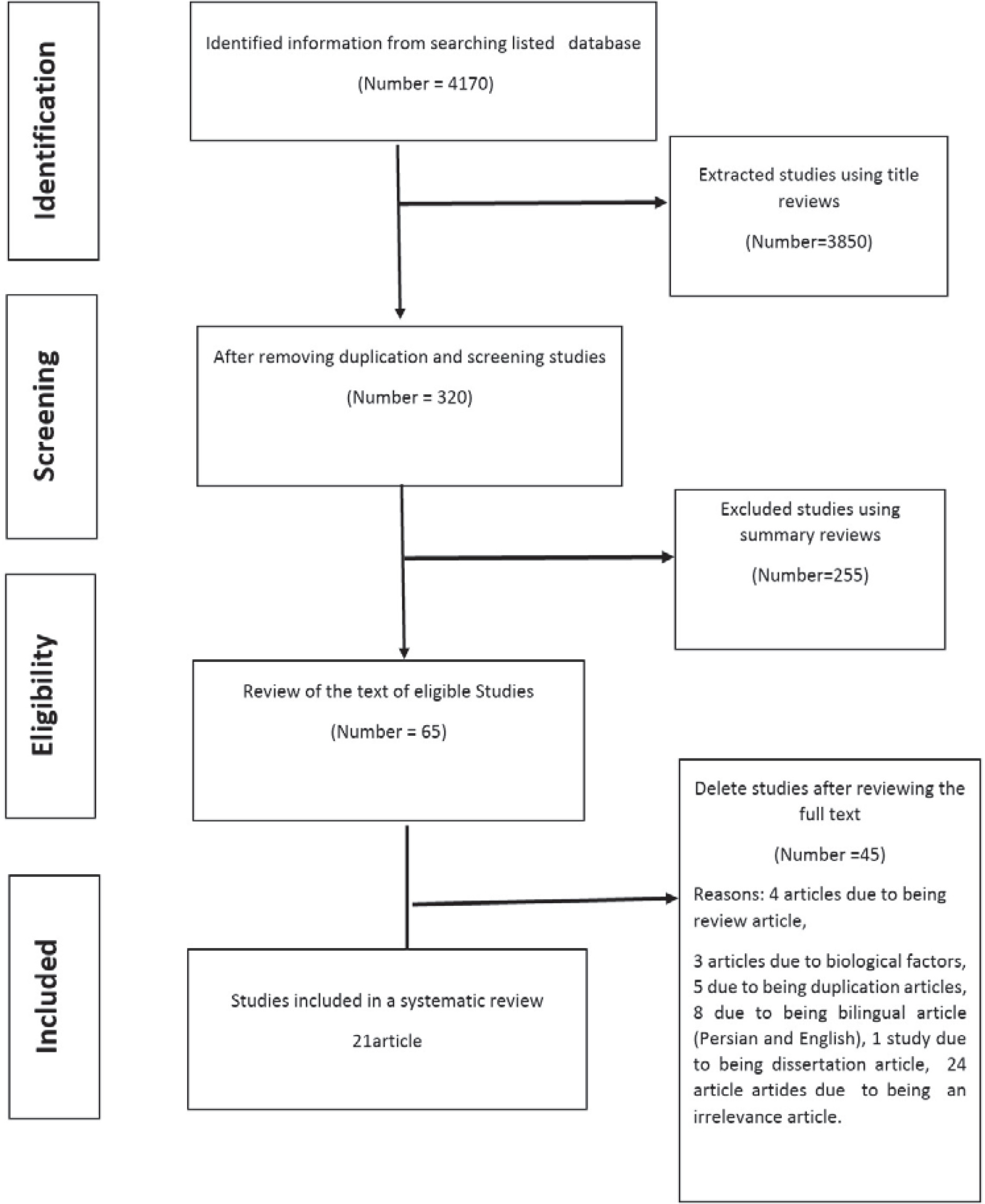
Table 1
Review of intervention studies and their results
| No. | Author, year, place | Sample size and features | Structures in these studies | Theory and model (types of interventions) | Results |
|---|---|---|---|---|---|
| 1 | Bakhtari Aqdam et al.20 2020 East Azerbaijan | 266 people 133 in Hashtrood city 133 in Qarah-Aghaj | Social support, perceived – sensitivity, intensity, and reward | Social-Ecological model Informal teaching methods (social networking, discussion of messages, problem solving and discussion of the initial negative consequences, teaching text messages, pictures and short videos to strengthen the perceived sensitivity in the Telegram group Emotional and instrumental support by managers, verbal encouragement for group members in the social environment, use of posters, intervention for 8 weeks | Social support structures Perceived sensitivity changed. The frequency of hookah smoking decreased in 72.6% of participants in the intervention group (6.3% in the control group). The duration of hookah smoking each time was reduced in 39.5% of the participants in the intervention group. |
| 2 | Basharian et al.21 2019 Iran | 102 people in public places and food managers | Attitude structures, subjective norm. Perceived –behavioral control and intent to reduce hookah supply | Theory of planned behavior, educational intervention Lecture method of the training program during 4 sessions in a month | Educational intervention led to a 25.1% decrease in the intention to supply hookah among the operators of the experimental group. Educational interventions based on the theory of planned behavior are effective in reducing the supply of hookah among operators of public places and food. |
| 3 | Basharian et al.22 2019 Hamedan, Iran | 94 people students | Collaborative dialogue structures Behavioral assurance Emotional transformation and performance for change | Multi-theoretical model structures Face-to-face and peer training Follow-up two months later | Hookah smoking decreased from 14.9% to 4.8% in the intervention group but no change was observed in the control group. The results of this study emphasized the effect of interventions on multi-theory model structures and the implementation of educational interventions for adolescents. |
| 4 | Joveini et al.23 2020 Sabzevar, Iran | 150 male students who smoke hookah | Perception of risk, expectation of consequences, self-efficacy of action, attitude, abstract norms, behavioral control and behavioral intention, health behavior approach | Theory of planned behavior, 45 minute intervention in 6 sessions for the intervention group | Educational intervention designed based on the theory of planned behavior and the motivational stage of the health behavior process approach is effective in creating the intention to quit hookah smoking in students. |
| 5 | Joveini et al.24 2013 Tehran, Iran | 90 male students of Tehran University of Medical Sciences | Attitudes, abstract norms, behavioral control and intention to reduce hookah supply | Theory of planned behavior (lecture) Follow-up two months later | There is a significant difference between the mean scores of attitude, behavioral intention, abstract norms and perceived behavioral control in the students of the experimental group compared to the control group after the educational intervention. In addition, the number of hookah smoking among students in the experimental group was significantly reduced compared to the control group after the educational intervention. |
| 6 | Bashirian et al.25 2020 Iran | 240 people students | Prototype Willingness attitude, behavior, intention, subjective norm | PWM model, use of electronic interventions, 5 e-learning sessions (videos, clips, e-booklets) Follow-up after 3 months | The mean score of PWM model before the educational intervention was similar in the intervention and control groups. But after the educational intervention, the mean score of positive attitude towards hookah was p=0.01, abstract norms p=0.01, positive perceptions towards people who smoke hookah p=0.004, intention p = 0.002. Behavioral tendencies p=0.017 decreased in the experimental group and the mean score of positive perceptions about the people who do not smoke hookah in this group increased. |
| 7 | Mahoozi et al.26 2017 Bushehr, Iran | 60 women who referred to medical centers of Bushehr University of Medical Sciences | Awareness, performance attitude | KAP, 8-week training intervention including training booklets, videos, slides, discussion, questions and answers Follow-up two months later | Awareness of 48% of the participants in the sessions about the carcinogenic effects of hookah was moderate. 100% of the participants were aware of 33.1% and their attitude towards hookah smoking was 100% positive, which was reported as 5% after the intervention. |
| 8 | Rajabalipour et al.27 2019 Kerman, Iran | 189 high school students | Self-efficacy, outcome expectations and environmental structures | Social cognitive theory, educational interventions included Questions and answers, group discussions and lectures Follow-up 4 months later | In the results of this study, although some structural scores showed a significant difference after the intervention, but no significant change occurred in the prevalence of WP hookah smoking. The effectiveness of educational interventions based on this theory may be guaranteed by greater focus and self-efficacy and environmental influences |
| 9 | Mojahed et al.28 2018 Zahedan, Iran | 140 pregnant women who smoke hookah | Self-efficacy motivational interview to quit hookah | Self-efficacy for quitting hookah 60–90 minute motivational interview sessions Follow-up two months later | The mean score of self-efficacy in both groups before the intervention did not show a statistically significant difference, while after the intervention, the self-efficacy score increased in the intervention group. Due to the fact that motivational interviewing has a positive effect on increasing the self-efficacy of hookah quitting, so the integration of this strategy in the care programs of pregnant women who use hookah is recommended. |
| 10 | Momenabadi et al.29 2015 Kerman, Iran | 80 male and female students living in the dormitory of Kerman University of Medical Sciences | Attitude score, subjective norm, and behavioral intention | Baznef model Training program (group discussion, question and answer, giving an educational CD to change attitudes and installing posters) Follow-up two months later | Attitude p=0.66 Subjective norm p=0.103 Behavioral intention p=0.13 There was no significant difference between the two groups before the intervention, but the results after the training showed a significant difference in the score of attitude, abstract norm and behavioral intention. Enabling factors in both groups before and after the intervention did not show a significant difference. |
| 11 | Ezati Rad et al.30 2015 Bandar Abbas, Iran | 128 women who smoke hookah at least once a day | Attitude, behavioral intention, internal norms and behavioral control | Theory of planned behavior, 4 sessions for group discussion, questions and answers, role playing, lectures Follow-up two months later | Designing an intervention based on the theory of planned behavior can act as an effective strategy to reduce hookah smoking among women. |
| 12 | Sotoudeh et al.31 2015 Bushehr, Iran | 127 women who smoke hookah in Bushehr | Awareness Perceived – barriers, benefits, sensitivity, severity; self-efficacy, nicotine dependence | Health belief model, educational interventions Follow-up three months later | Before training, the two groups were the same in terms of demographic characteristics and knowledge status of health belief model and did not differ significantly. After training, the average of the structures of the pattern of health belief and awareness in the intervention group increased and the number of hookah smokers in the intervention group decreased. |
| 13 | Sadeghi et al.32 2020 Iran | 280 people | Knowledge Perceived – severity, susceptibility, cost. Response efficiency | Educational campaign Training and information about hookah and its harms | There was a significant change in the mean scores of knowledge and perceived susceptibility, perceived severity, response efficiency, self-efficacy, rewards, fear and protection motivation after the HEHC, but there was no significant difference in the structure of perceived cost. |
| 14 | Jawad et al.33 2015 London, UK | 214 people | Awareness | Communication model Intervention using social media (Facebook, Twitter, YouTube) and a campaign website Follow-up 9 months later | Facebook attracted fans of the campaign, but YouTube attracted opponents. Twitter enabled the most corporate communication, but Facebook was the most interactive. Facebook users commented more on (the reality of hookah smoking). As the posting rate increased, followers also increased. The video received 42819 views from all over the world and received 218 comments (86% from hookah fans). |
| 15 | Asfar et al.34 2014 Syria | 50 adults who smoked hookah 3 times a week in the last year and they were interested in quitting hookah They did not smoke cigarettes | The short program included a 45-minute training session and 3 follow-up phone calls. The intensive program included 3 training sessions that lasted 45 minutes each session, and 5 follow-up phone calls made by a doctor to behavior quitting. | 30% of participants adhered to treatment that was not changed by the treatment group. The proportion of participants in brief and intensive interventions with long-term abstinence in the 3-month evaluation were 30.4% and 44.4% (p=0.31), respectively. Adherence to treatment, readiness, self-confidece and unemployment (p<0.05) were predicted. | |
| 16 | Dawood and Obaid35 2018 Baghdad, Iraq | 132 high school students | Attitude Perception of danger | 30–40 minute educational interventions in 2 sessions including group discussion and lecture Follow-up 3 months later | There was a significant difference in the mean score of hookah smoking perception in the intervention group before and after the intervention. There was a significant improvement in the mean score of attitude about the side effects of hookah smoking after training in the intervention group. |
| 17 | Leavens et al.36 2018 Midwest, USA | 109 students | Awareness, belief, performance | KAP Two sessions of educational intervention on hookah side effects Follow-up 3 months later | After educational interventions in the intervention group, knowledge about hookah side effects increased p<0.0001 Perception of risk improved p = 0.0047 But after 3 months of follow-up, there was no significant difference between the intervention and control groups in hookah smoking. |
| 18 | Mays et al.37 2020 USA | 234 people in the age group of 18–30 years | Assess fear, threat, behavioral desire | Receive messages, text, images including the dangers of hookah smoking, side effects, harms caused by hookah, hookah addiction. | Educational interventions were performed on the side effects of hookah, comparison of pathogenicity of hookah and smoking, severity of addiction, comparison of hookah addiction to smoking. The results after the intervention showed that there was a statistically significant difference between the scores of perceived complications and perceived addiction in the intervention group compared to the control group. |
| 19 | Johnson and Mays38 2020 USA | 601 young hookah smokers | Intention, motivation, belief | Received messages randomly through social networks. Advertising messages related to hookah and messages related to the dangers of hookah. | The results showed that warning messages about the dangers of hookah have a great impact on young people. These messages increase the motivation of young people to quit hookah. In fact, the results showed that related messages about the dangers of hookah via Instagram could offset the impact of advertising messages about tobacco and hookah smoking. |
| 20 | Johnson et al.39 2019 USA | 156 hookah smokers in the age group of 18–30 years | Beliefs, attitudes | KAP study Multimedia message about the dangers of hookah smoking among young people. | Before viewing the text message, most participants had a misconception about hookah. But after observing the messages about the dangers of hookah smoking, the results showed that the participants accepted the messages and it caused concern in them. Examining the effectiveness of MMS as a strategy to prevent and reduce hookah smoking among young people is essential. |
| 21 | Lipkus et al.40 2014 USA | 203 adult hookah smokers 90 people in the intervention group 112 people in the control group | Awareness, belief, performance | KAP Two web-based sessions were conducted and users received information about the side effects of tobacco use. Follow-up 6 months later | After the intervention, participants who received information about hookah side effects showed a higher perceived risk p=0.009. They showed more concern about addiction. Also in this study, 62% of the participants in the intervention group reported that they had quit hookah smoking. |
RESULTS
Of the total articles included in this study, 13 studies were from Iran20-32, 1 article from the UK33, 1 from Syria34, 1 from Baghdad35, 1 from the Midwest36 and 4 other studies from the United States37-40.
In terms of period, 5 studies were conducted in 2019–202020,25,32,38,39, 4 studies in 201821,22,35,36, 2 in 201723,28, 5 in 2015–201626, 27,29,30,36, 4 studies in 201433,34,37,40 and 1 in 201124.
Two interventional studies were designed using the PWM25,33, 1 study used the social-ecological model20, 1 study used the multi-theory model22, 4 studies used the theory of planned behavior 21,23,24,30, 3 studies used the KAP study26,36,37, 1 study used social cognitive theory27, 1 study used health belief model31, and 1 study used the BASNEF model29 in designing interventions.
One study emphasized the effects of interventions to increase self-efficacy with motivational interviews28. In one study, interventions were performed using a communication and social media model (Facebook, Twitter, and YouTube) and a campaign website34. Other studies have used educational programs to change attitudes and awareness to reduce the prevalence of hookah smoking38.
Sample size
In terms of sample size, 5 studies had a sample size between 200 and 300 people20,25,32,33,40, one study had a sample size of 600 people38, and other studies had a sample size between 50 and 190 people21-24, 26-31,34,35,37,39. Among the reviewed articles, the target group in 5 studies was students, 1 study was conducted on public places and food managers25. In 3 studies, the target group was students23,24,29, and 4 studies were conducted on women26,28,30,31. Other studies were performed among people in different age groups.
Interventions performed to prevent and reduce hookah smoking
All studies indicated that the interventions effectively reduced hookah smoking behavior, except in 1 study where no change in hookah smoking behavior was observed after the educational intervention37. The results of two studies showed that web-based interventions could effectively control hookah smoking25,40. One study emphasized the role of the BASNEF model and the effect of structures (attitude, abstract norm, intention). Still, the results of this study did not show a change in the structure of enabling factors after training29. Five studies referred to the design of educational intervention based on the pattern of planning behavior. In this study, the effect of the intervention on the content of self-efficacy was shown. The study emphasizes the role of attitude and the effect of educational interventions on the structure of attitude.
In one study, the interventions were designed based on the social-ecological model. This study showed that the frequency of hookah smoking decreased in 72.6% of participants in the intervention group. The duration of hookah smoking in each session decreased in 39.5% of the participants in the intervention group. In one study, a multi-theoretical model was used to design interventions. Educational interventions were designed based on participatory construction, behavioral confidence, behavioral transformation, and performance for a change. hookah smoking decreased from 14.9% to 4.8% in the intervention group, but there was no change in the control group.
The results of this study emphasized the implementation of educational interventions based on the multi-theory model for adolescents. In one study, interventions were designed through Instagram and mobile multimedia messages about the dangers of hookah smoking among young people. Before viewing a text message, most participants had misconceptions about the dangers of hookah, but the results showed that the participants accepted the messages, and it had caused concern. In fact, the results showed that young hookah smokers are receptive to mobile multimedia messages, and testing the effectiveness of MMS as a strategy to prevent and reduce hookah smoking among young people is essential.
Table 2 shows the quality assessment of the studies. Out of 21 studies, 17 studies were weak in terms of quality, 4 studies were medium, and there were no high-quality studies.
Table 2
The quality assessment of the studies, out of 21 studies, 17 studies were weak in terms of quality, 4 studies were medium in terms of quality and there were no high-quality studies
Table 3 shows the calculation of the kappa coefficient. Kappa coefficient was used to examine the agreement between the two researchers during the quality assessment of the studies. The agreement between the two researchers was based on the 5 components of the EPHPP tool. The agreement between the researchers for the sample attribution (0.694) was good, and for other components of the agreement, it was perfect (0.80 to 1.00).
Table 3
Calculation of kappa coefficient
DISCUSSION
Due to the increasing prevalence of hookah smoking and the lack of sufficient interventions in this field, it is necessary to study the interventions and determine their impact on most hookah smokers. Therefore, the present study was performed to assess the effect of interventions to prevent and reduce hookah smoking. After reviewing the articles by the researchers, 21 articles were finally identified for evaluation in this study. The sample size of most studies was small (less than 200 people), and the outcomes measured in the studies were primarily report-based. In the studies, according to the objectives of the studies, educational programs and interventions were designed based on patterns and models of health education.
This issue can be one of the limitations of the prevention and control of hookah smoking. According to the results of the studies, most of the studies examined the design of interventions based on individual and interpersonal factors affecting the tendency to smoke a hookah. A few studies examined organizational and community factors in the smoking hookah. In most studies, educational interventions had a significant impact on the correction of individual factors such as attitudes, awareness, positive perceptions towards the hookah smoker and behavioral tendencies.
The results of some studies showed the effect of web-based educational interventions and the use of videos and images in reducing and controlling hookah smoking. In fact, comparing the educational method of using the educational booklet and the use of educational clips also showed that movies and animations, with PowerPoint color animations and educational slides with messages, colors and happy images, engage people’s imagination and create a kind of excitement that this can be the main factor in the effectiveness of educational clips over textbooks41-43. The results showed that in most studies, educational interventions were effective in correcting a positive attitude towards hookah smoking. Also, the results of a study by Heidernia et al.44 showed that the implementation and design of e-learning packages is effective in preventing smoking in adolescents. Also, the results of the present study showed that the use of social networks to implement interventions will help the process of controlling hookah smoking. The study of Khazaee-Pool et al.45 showed that the main sources of information about the risks of a disease were social networks (Telegram, WhatsApp, Instagram, Twitter, Facebook, email), respectively, which shows the high impact of new technologies in disseminating information related to risks and diseases. The findings of the present study showed that educational interventions about the side effects of hookah smoking and comparing the pathogenicity of hookah and smoking and the severity of hookah addiction are among the educational programs that can help reduce hookah smoking46. Evidence also shows that educational interventions by negating positive perceptions about hookah smoking will cause people who have positive perceptions of hookah smoking to start worrying about the future.
Curtis et al.47. showed in their study that electronic interventions reinforce negative attitudes toward smoking. Studies by Joveini et al.48, Shegog et al.49, and Hopfer et al.50 showed that tobacco prevention programs are effective in reducing positive attitudes toward tobacco.
The study by Maziak et al.7 showed a positive attitude towards hookah smoking among Syrian women, which is a matter of concern. Examining the hookah dependence syndrome is necessary to change attitudes. Therefore, researchers must pay attention to this structure of attitudes to improve interventions and develop strategies to prevent smoking.
In addition, the results of the present study emphasize the role of educational interventions in increasing the self-efficacy structure, which was one of the essential structures in reducing hookah smoking.
Numerous studies have shown that self-efficacy plays a vital role in smoking cessation. People with high levels of self-efficacy are more likely to be more successful at avoiding hookah smoking. People with higher self-efficacy expectations are more likely than individuals with lower efficiencies to seek suitable solutions to solve problems. For example, Grembowski51 and O’Leary52 found in their research that people with high self-efficacy expectations were more likely to control harmful behaviors (such as obesity) and self-destructive behaviors such as smoking. People with high self-efficacy avoid self-destruction and experience less anxiety and depression. In fact, designing interventions such as verbal persuasion can increase a person’s self-efficacy53.
The results of the study emphasized the role of social support. Social support may reduce the detrimental effects of stress in two ways. First, social support reduces stress by vaccinating a person against experiencing stress before it occurs. If one has a rich social network of counseling, resources facilities, and financial aid, the potential pressures will not cause concern and anxiety. Second, social support networks act as a shield against stress. If a person can refer to the social network during stress, it allows him/her to evaluate life events as less threatening. Finally, social support can increase the resistance of individuals to the negative effects of stressors and thereby improving a person’s mental health54.
In the design of the five studies, the structures of planned behavior theory were used, and the role of factors such as abstract norms was emphasized. Since hookah is a collective phenomenon, one of the factors that significantly impact hookah smoking is the role of friends and family. Having family and friends who smoke hookah increases a person’s desire to smoke hookah55.
The role of mental norms and the influence of peers in adolescents should be considered more than other age groups. In this regard, the strategies of the present study, such as teaching the skills of saying no to friends, play an essential role in preventing smoking hookah44. Thus, under the pressure of others, there may be stronger willingness to engage in risky behavior without prior intention. Therefore, adolescents should learn communication skills such as ‘refusal’ and ‘saying no’ and should not respond emotionally to the issue of smoking and its suggestion by friends.
There was not much emphasis on enabling factors in the environment in the study of interventions. A study was designed based on the BASNEF model, and the enabling factors did not change significantly after the educational intervention in the intervention and training groups. These results indicate that more attention should be paid to the environment and access to hookah at home and work56.
The presence of hookah in cafes and restaurants and access to hookah for people under 18 years has made the cafe an attractive and motivating place, and it is a cheap way for young people to spend free time.
This may be due to the focus on marketing strategies and the lack of hookah prohibition laws in public places57. Rules for banning hookah in cafes and restaurants, raising hookah prices, banning hookah smoking for people under 18 years, and educating people about identifying tempting advertisements, are some of the interventions that can help prevent hookah smoking56,57.
In fact, the results of the present study showed that designing interventions, in the framework of health education and health promotion models, can be an effective strategy to reduce smoking, and, together with new educational methods such as web-based interventions, the most important ways to reduce positive attitudes toward hookah smoking.
Our suggestions according to the results of the present study include: using different theories and behavioral and social models in designing studies; strengthen prevention activities against hookah smoking and using operational strategies and effective methods of each determinant; the establishment of counseling centers; and using people that are familiar with operational strategies, to increase confidence in personal ability to change hookah smoking behavior.
CONCLUSIONS
Most of the studies examined individual and interpersonal factors affecting the prevention and reduction of hookah smoking. In contrast, hookah smoking is a multifaceted issue, and interventions should be designed at different levels (multilevel).
Considering the effect of various interventions and the use of patterns and theories of health education can be very helpful in changing and modifying some factors affecting the tendency to hookah smoking.