

INTRODUCTION
Tobacco remains the single most preventable risk factor that acts against present and future generations, having devastating health, social, environmental and economic consequences through its consumption and exposure1. It is one of the main public health problems killing over 8 million people, with 9 in 10 as a result of direct tobacco use, and 1 in 10 due to exposure to tobacco smoke2. It is a challenge to public health as 8 in 10 of 1.3 billion adult smokers are located in low- and middle-income countries including Ghana. This high level of tobacco consumption and exposure leads to high tobacco-related morbidity and mortality as a result of high level tobacco addiction3 and poverty within the immediate families of the tobacco users due to the diversion of household money from buying basic needs, such as food and shelter, to tobacco purchases4. Tobacco addiction and continuous use also lead to increased healthcare costs as a result of increased tobacco-related disease5. It is well documented that tobacco and tobacco products have no safe level of exposure. Cigarettes are the most commonly used6 tobacco product followed by other types such as waterpipe tobacco (shisha), smokeless tobacco products, cigars, cigarillos, roll-your-own tobacco, pipe tobacco, bidis, and kreteks7. Waterpipe tobacco smoking (hookah, shisha, narghile) use is on the rise and has received attention from public health researchers and practitioners due to its fastgrowing use by and appeal to some populations8,9. This high demand for waterpipe (shisha) use, especially by youth can be attributed to the deceptive and aggressive marketing strategies of the tobacco industry, falsely presented as safer form of cigarette smoking6,9. Studies have confirmed that most shisha smokers are unaware of the harmful health effects of shisha smoking10,11 being deceived that the toxins in the smoke are filtered out by the water in the pipe12. Shisha contains the same chemicals and substances as cigarettes including carbon monoxide (CO), tar, nicotine and highly toxic and carcinogenic substances. Shisha has as well a higher level of heavy metals such as arsenic, nickel, cobalt, chromium, lead, and cadmium, than cigarette smoke13. As a result of the social interactions and long duration of shisha sessions, users and secondhand smokers are being exposed to greater levels of nicotine and CO than cigarette smoking and the amount inhaled can be more than ten times higher13.
The effects of tobacco use on the rather fragile economies of LMICs, including Ghana, may go unnoticed as a result of the paucity of data, yet tobacco use is significantly increasing healthcare costs from tobacco-related diseases and loss of human resources to morbidity and mortality14. Ghana is considered to be at the beginning of the tobacco epidemic compared to other African countries15. Despite the low prevalence of tobacco use, about 50 men and 16 women die every week as a result of tobacco-related diseases in Ghana. This constitutes 2.7% and 1.0% of the annual deaths among men and women, respectively16. The situation of the youth in Ghana is not so different from that of the adults, where the current report from the Global Youth Tobacco Survey (GYTS) shows that close to 9% of the youth in Junior High Schools (JHS) aged 13–15 years are currently using tobacco products, and 1.3% are currently smoking shisha with the greater proportion among girls9,17. This study, therefore, assessed the predictors of tobacco use (cigarettes/shisha) in two communities in Accra, to provide data that will support the development of prevention strategies and policies for Ghana.
METHODS
Study site
The study was conducted in one urban slum (Nima) and one urban community (Osu) in the capital of Ghana, Accra. The Nima community is associated with slum settlement and lacks basic needs such as potable water supply, and faced with waste management issues. The community also has a high population of migrant workers from other regions of Ghana mostly from the three northern regions. The Nima community is among the areas known to indulge in the use of addictive substances including weeds, cannabis and tobacco, mostly among the youth as a result of high level of unemployment18. Osu on the other hand was a traditional coastal fishing settlement predominantly of the Ga ethnic group. However, it has grown into a network of cosmopolitan neighborhoods, with Oxford Street serving as the main center of the community. As a result of the variety of activities in the area such as cinemas, boutiques, cafes, restaurants, street food stalls, and art and craft stalls, it draws many people especially the youth and expatriates.
Sample size calculation
The study used the 2010 Ghana population census data19 to obtain the populations of households in the two communities, about 122000 and 184000 for Osu and Nima, respectively. By employing a random sampling technique, we used Slovin’s formula to determine the sample size with a 5% margin of error. The formula uses the study population (N) and margin of error (e) to determine the sample size (n). A total of 389 respondents were required for the study. Of the 389 respondents, 135 (approximately 35% of the respondents) and 254 (approximately 65% of the respondents) were selected from Osu and Nima communities, respectively. Study respondents were aged ≥18 years.
Using the 2010 Population and Housing Census of Ghana19 as the sampling frame, 135 households were randomly selected from Osu and 254 from Nima. Only one respondent was interviewed in each household. Up to three repeat visits were made to households when no person aged ≥18 years was present at the first visit. After three visits, a household was replaced with another randomly selected household within the sample frame. Also, nonresponding households were replaced with another randomly selected household within the respective sample frames. Subsequently, respondents from 389 households (135 from Osu and 254 from Nima) participated in the study.
Between May and June 2017, trained research assistants visited the selected households and explained the study and obtained informed consent through a signature or thumbprint, as appropriate. Respondents were assured of confidentiality of the information collected. Face-to-face interviews were performed using a structured questionnaire.
Data collection
A structured questionnaire20 was used to collect data from respondents in the two selected communities. Face-toface interviews were conducted, by the trained research assistants, among all respondents who consented to take part in the survey. Data on the use of cigarettes and other tobacco products, exposure to secondhand smoke, shisha smoking, electronic cigarette use, as well as demographic information of respondents were collected.
Study measures
Cigarette smoking status
We assessed the respondents’ tobacco smoking status with two questions: ‘have you ever smoked a cigarette, even if it is one or two puffs?’ and ‘during the past 30 days, on how many days did you smoke cigarettes?’. Those who responded negatively to the two questions were classified as never smokers and former smokers, respectively. Both never and former smokers were categorized as current non-smokers.
Tobacco smoking status
We also assessed respondents smoking status with the question: ‘have you ever smoked tobacco products other than cigarettes, even if it is one or two puffs?’. Those who chose ‘yes’ and ‘no’ were classified as ever tobacco smokers and never tobacco smokers, respectively.
Willingness to quit smoking
We assessed respondents’ willingness to quit smoking by asking them three questions: ‘do you want to stop smoking now?’, ‘do you ever try to stop smoking?’ and ‘do you think you could stop if you wanted to?’ Those who responded ‘yes’ to all three questions were classified as willing to quit, those who responded ‘no’ or ‘don't know’ were classified as not willing to quit smoking.
Exposure to secondhand smoke
We also assessed respondents’ exposure to secondhand smoke in their communities by asking them: ‘do you think you are exposed to secondhand smoke?’ and ‘do you think the smoke from other people’s tobacco smoking is harmful to you?’. Respondents who answered ‘yes’ showed an awareness of the harmful effects of tobacco use in their communities. Also, a further question included ‘how many days per week are you exposed to secondhand smoke in indoor or outdoor public places (public toilets, clubhouses, schools, shops, restaurants, shopping malls, movie theatres)?’.
Shisha use status
We also assessed shisha use among respondents in the community as follow: ‘have you ever heard of shisha?’, ‘have you ever used shisha?’, ‘how often do you smoke shisha?’, ‘do you think the smoke from other people’s shisha smoking is harmful to you?’ and ‘the last time you smoked shisha, where did you smoke it?’. Respondents who never heard of shisha were classified as non-shisha users, ones who heard and never used it before were classified as ever users, while respondents who used shisha during the last month before proceeding with the study were classified as current shisha users.
Statistical analysis
Frequencies and percentages were used to describe the distribution of the demographic characteristics of study respondents. The prevalence of ever and current use of cigarettes, shisha, and electronic cigarettes is presented with 95% confidence interval. We explored the difference in ever use of cigarettes, shisha, and electronic cigarettes, by sex and age. Chi-squared test was used to assess the association between the demographic characteristic of respondents and current cigarette and shisha smoking. Using a composite variable for current cigarette and/or shisha smoking, logistic regression analysis was performed to assess the association between demographic characteristics of respondents and current cigarette/shisha use. First, univariate logistic regression was used to assess the independent association of each of the demographic characteristics included in the study. Variables in the univariate analysis with p<0.20 were included in a multivariate logistic regression model. Also, given our interest in age and sex, these variables were included in the multivariate logistic regression model regardless of their statistical significance in the univariate analysis. A statistically significant level of 5% was used for the multivariate analysis. STATA version 14 was used for the statistical analysis.
Ethical approval for the study was obtained from the Ghana Health Service Ethics Review Committee (GHSERC017/08/17). Also, permission was sought from the Municipal Assembly before the conduct of the study. Consent was obtained from all participants after a detailed explanation of the study objectives, procedures, risks, and benefits have been provided in the presence of witnesses before any interview. Respondents were fully informed that their participation was voluntary and they could decide not to answer a question or withdraw from the study entirely, and data would be anonymously recorded.
RESULTS
Description of study participants
Table 1 describes the demographic characteristics of the 389 respondents. There were more male participants than females, 68.1% versus 31.9%. Most of the study respondents 246/389 (63.3%) were aged <36 years. Likewise, more than half of the respondents had education ranging from senior high school to tertiary education, and 19.0% of the respondents were unemployed.
Table 1
Demographic characteristics of study respondents (N=389)
Ever use of cigarettes, shisha, and e-cigarettes by sex and age
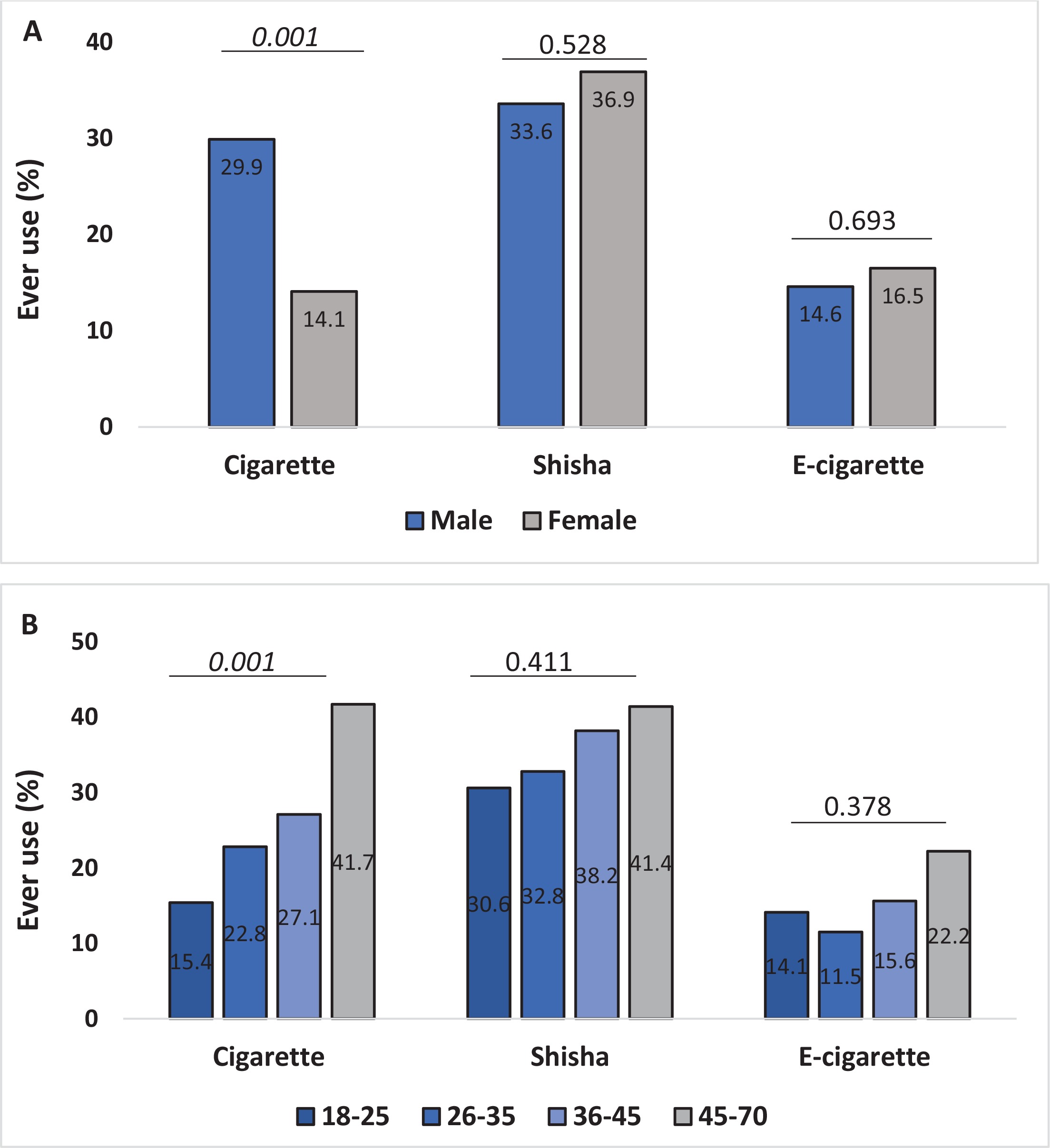
The prevalence of ever smoking cigarettes, shisha and electronic cigarettes was 24.9% (95% CI: 20.8–29.5), 34.6% (95% CI: 30.0–39.6) and 15.1% (95% CI: 11.3–19.8), respectively. The distribution of ever-smokers of cigarettes, shisha, and electronic cigarettes by sex and age is shown in Figure 1. There was a significant difference in the proportion of respondents who have ever smoked cigarettes, by sex and age. Compared to females, more males have ever smoked cigarettes. Also, the percentage of respondents who have ever smoked cigarettes was higher among older participants.
Demographic characteristics of current cigarette or shisha users
The demographic characteristics of respondents by current cigarette and shisha use are presented in Table 2. The prevalence of current cigarette use was 13.1% (95% CI: 10.1–16.9), current shisha use 10.3% (95% CI: 7.6–13.7) and 19.5% (95% CI: 15.9–23.8) smoked either cigarettes or shisha. Out of the demographic variables included in the analysis namely, place of residence, sex, age, marital status, education level, and employment status, only marital status was statistically significantly associated with cigarette smoking. Cigarette use was more prevalent among married/married before/co-habiting respondents compared to respondents who were single, 16.8% versus 9.4%. On the current use of shisha, only the sex of respondents was of significant importance. Compared to females, shisha use was more prevalent among males, 13.6% versus 3.2% (Table 2).
Table 2
Distribution of current cigarette and shisha smokers by demographic characteristics
| Characteristics | Current cigarette smoking | Current shisha smoking | ||||
|---|---|---|---|---|---|---|
| Smokers (n=51) | Non-smokers (n=338) | Smokers (n=40) | Non-smokers (n=349) | |||
| n (row %) | n (row %) | p | n (row %) | n (row %) | p | |
| Residence | ||||||
| Urban | 17 (12.6) | 118 (87.4) | 0.825 | 14 (10.4) | 121 (89.6) | 0.967 |
| Urban slum | 34 (13.4) | 220 (86.6) | 26 (10.2) | 228 (89.8) | ||
| Sex | ||||||
| Male | 33 (12.5) | 232 (87.5) | 0.574 | 36 (13.6) | 229 (86.4) | 0.001 |
| Female | 18 (14.5) | 106 (85.5) | 4 (3.2) | 120 (96.8) | ||
| Age (years) | ||||||
| 18–25 | 10 (8.2) | 112 (91.8) | 0.147 | 12 (9.8) | 110 (90.2) | 0.257 |
| 26–35 | 16 (12.9) | 108 (87.1) | 18 (14.5) | 106 (85.5) | ||
| 36–45 | 11 (15.7) | 59 (84.3) | 4 (5.7) | 66 (94.3) | ||
| 46–70 | 14 (19.2) | 59 (80.8) | 6 (8.2) | 67 (91.8) | ||
| Marital status | ||||||
| Married/married before/co-habiting | 33 (16.8) | 164 (83.2) | 0.031 | 15 (7.6) | 182 (92.4) | 0.079 |
| Single | 18 (9.4) | 174 (90.6) | 25 (13.0) | 167 (87.0) | ||
| Education level* | ||||||
| No, primary, JHS, middle | 30 (16.7) | 150 (83.3) | 0.137 | 21 (11.7) | 159 (88.3) | 0.582 |
| Senior high school/vocational | 14 (9.5) | 134 (90.5) | 12 (8.1) | 136 (91.9) | ||
| Tertiary | 6 (10.9) | 49 (89.1) | 5 (9.1) | 50 (90.9) | ||
| Employment status | ||||||
| Yes | 38 (12.1) | 277 (87.9) | 0.207 | 29 (9.2) | 286 (90.8) | 0.149 |
| No | 13 (17.6) | 61 (82.4) | 11 (14.9) | 63 (85.1) | ||
Association between demographic characteristics and cigarette and/or shisha smoking
Seventy-six respondents (19.5%; 95% CI: 15.9–23.8) were current smokers of either cigarettes or shisha. The results of the association between the demographic characteristics of the respondents and cigarette/shisha use are presented in Table 3. Sex, age, education level, and employment status, were included in the multivariate logistic regression analysis. In the multivariate analysis, only employment status was significantly associated with cigarette or shisha use. The odds of cigarette/shisha use for respondents who had no employment were 2.3 times the odds for those who had employment (OR=2.30; 95% CI: 1.19–4.44, p=0.013).
Table 3
Association between demographic characteristics and cigarette/shisha smoking
| Characteristics | Smokers (n=76) n (%) | Non-smokers (n=313) n (%) | OR (95% CI) | p | AOR (95% CI) | p |
|---|---|---|---|---|---|---|
| Residence | ||||||
| Urban | 25 (18.5) | 110 (81.5) | 1 | 0.711 | ||
| Urban slum | 51 (20.1) | 203 (79.9) | 1.11 (0.78–1.57) | |||
| Sex | ||||||
| Male | 55 (20.8) | 210 (79.2) | 1 | 0.371 | 1 | 0.565 |
| Female | 21 (16.9) | 103 (83.1) | 0.78 (0.54–1.12) | 0.84 (0.47–1.51) | ||
| Age (years) | ||||||
| 18–25 | 18 (14.8) | 104 (85.2) | 1 | 0.345 | 1 | 0.198 |
| 26–35 | 29 (23.4) | 95 (76.6) | 1.76 (1.15–2.70) | 2.20 (1.07–4.52) | ||
| 36–45 | 13 (18.6) | 57 (81.4) | 1.32 (0.79–2.20) | 1.78 (0.75–4.23) | ||
| 46–70 | 16 (21.9) | 57 (78.1) | 1.62 (1.00–2.64) | 1.69 (0.72–3.96) | ||
| Marital status | ||||||
| Married/married before/co-habiting | 39 (19.8) | 158 (80.2) | 1 | 0.896 | ||
| Single | 37 (19.3) | 155 (80.7) | 0.97 (0.70–1.34) | |||
| Education level* | ||||||
| No, primary, JHS, middle | 41 (22.8) | 139 (77.2) | 1 | 0.186 | 1 | 0.251 |
| Senior high school/vocational | 22 (14.9) | 126 (85.1) | 0.59 (0.41–0.86) | 0.60 (0.32–1.11) | ||
| Tertiary | 10 (18.2) | 45 (81.8) | 0.75 (0.46–1.25) | 0.73 (0.33–1.61) | ||
| Employment status | ||||||
| Yes | 55 (17.5) | 260 (82.5) | 1 | 0.040 | 1 | 0.013 |
| No | 21 (28.4) | 53 (71.6) | 1.87 (1.28–2.74) | 2.30 (1.19–4.44) |
DISCUSSION
We sought to assess the predictors of tobacco use (cigarettes/shisha) among two communities in two districts in Accra, to provide data that will support intervention and prevention policies in Ghana. Our findings show that current cigarette use was 13.1% (95% CI: 10.1–16.9), current shisha use 10.3% (95% CI: 7.6–13.7) and 19.5% (95% CI: 15.9–23.8) smoked either cigarettes or shisha. The cigarette smoking prevalences in the two communities are a little above the national prevalence of 10% among adults aged 15–49 years21. There are no nationally representative data on shisha however, the studies conducted reported varying prevalences22–24 including the youth prevalence of 1.3%9. Studies on waterpipe use or shisha in the African region are few. Our findings on shisha use differ from those of a related study in a poor urban community in Johannesburg which reported 60% of high school students ever used, while 20% were daily users25. Similar studies conducted in Nigeria and Rwanda (Kigali) reported a shisha prevalence of 7.1%26 and 20.8%27, respectively.
The reasons for the use of shisha were not different from other findings where participants believed shisha is a safer alternative to cigarette smoking, and used it out of curiosity and peer influence23,24,26,27. Shisha smoking has emerged in Ghana and gradually has become a public health issue that needs immediate response from policy providers and must be effectively regulated like any other tobacco product.
In the multivariate analysis, only unemployment was found to be significantly associated with higher odds of smoking cigarettes and/or shisha. Other studies28,29 have reported similar results. In a study conducted in Sri Lanka30, employment and monthly income were found to be associated with tobacco use. Similarly, in a Korean study, unemployment was found to be a significant risk factor for failure to quit and smoking relapse31, which agrees with our findings. Since unemployment is a significant risk factor for failure to quit, it is suggested that those with no employment smoke more and are less likely to quit. A related study in Ghana suggests that public policies for the promotion of higher educational achievement and improvement in income are important in smoking reduction and cessation32. Substance abuse can be challenging for several reasons including dependence on toxic substances, which usually affect health and also employment status33. Despite this, the cross-sectional evidence is only associative and does not address the issue of causality, hence further studies are recommended, especially longitudinal. In a similar study by Abdel-Hady and El-Gilany34 in Egypt, an association between tobacco use and education and also sex was found, which is not consistent with our findings. According to them, lower education level is a significant independent predictor for current smoking in older people, which is also consistent with other studies35,36. Also in the United States, adults with lower levels of education, who also are unemployed, or live near or below the US Federal poverty level are considered to have low socioeconomic status (SES) and turn to smoking cigarettes more37. Our study could not establish these associations except that of employment, hence the need for further studies.
Our study suggests attention should be given to social inequality in smoking since unemployment could predict smoking uptake and decrease quitting. When this happens, it can derail government efforts in curbing tobacco prevalence in the country. Also, it is suggested that attention is given to specific populations, especially the unemployed, for targeted education on the harmful effects of tobacco use. This can be done alongside the implementation of comprehensive smoke-free laws and other strategies, which are proven to reduce smoking prevalence and adverse health outcomes38,39.
Strengths and limitations
The study had some limitations which include the sample size which was only limited to two districts that are not representative of the nation and not generalizable. Also, since this was a cross-sectional survey that relies on selfreports, there is the possibility that socially desirable responses were given and that there might have been recall bias. Nevertheless, it is expected that the findings will form the basis for further nationally representative studies. As the data were cross-sectional, we cannot make firm conclusions regarding the causal pathway connecting unemployment and smoking.
CONCLUSIONS
When smoke-free laws and key policies are implemented, attention to social inequality in smoking must be considered to avoid derailing government efforts in tobacco control. Also, policy formulation to prevent smoking uptake must take into account specific populations to have maximum effect, especially people who are not employed.