


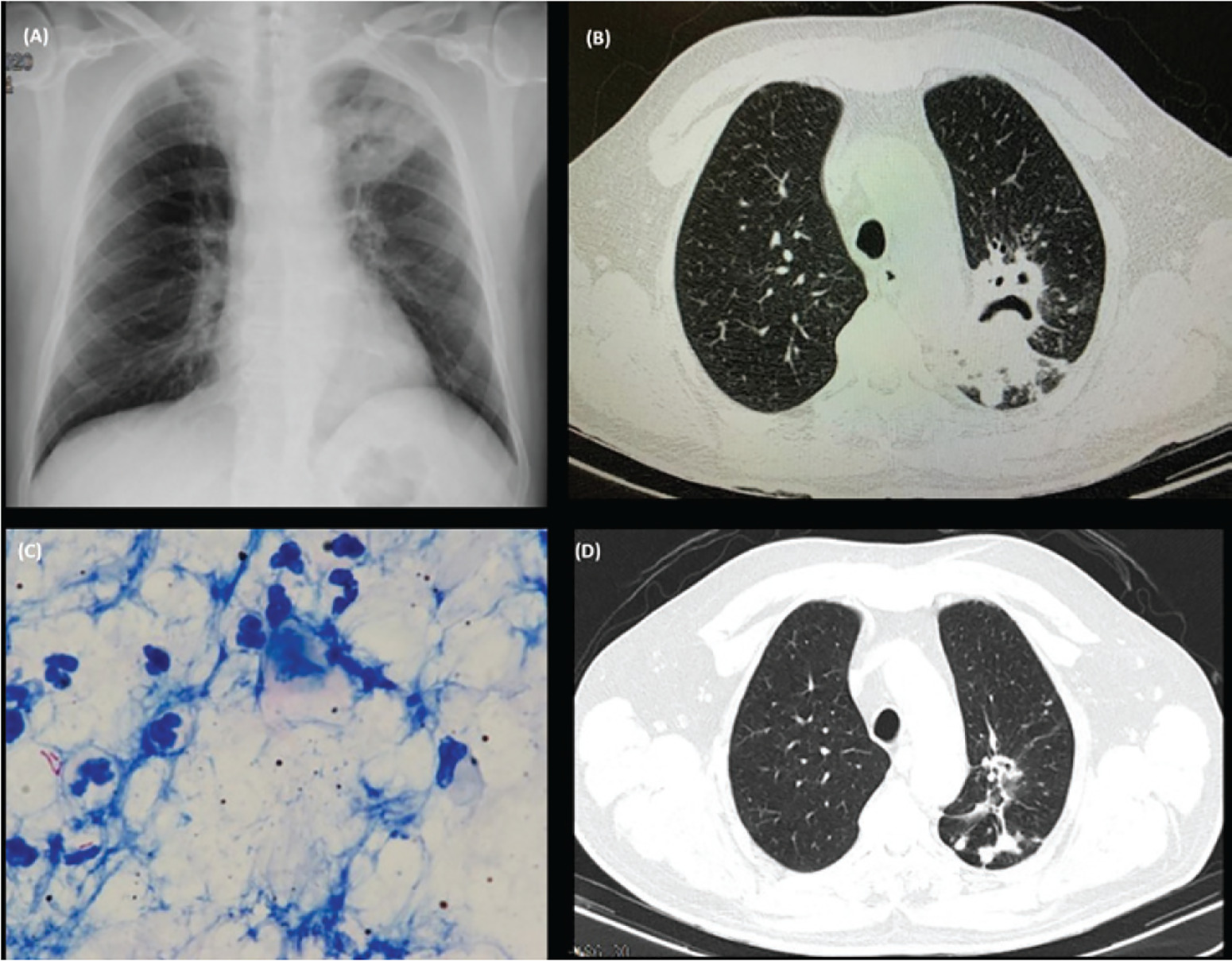
A 67-year-old male was presented to the Emergency Department with mild hemoptysis, productive cough, asthenia, and weight loss for several months. In terms of comorbidities, the patient reported having type 2 diabetes, hyperuricemia, and hypertension. His usual medication was as follows: allopurinol 100 mg, pantoprazole 20 mg, furosemide 20 mg, amlodipine 5 mg, and candesartan 8 mg. The patient was not taking any anticoagulants or antiplatelet agents. Laboratory tests were performed and revealed the following results: PCR 2 mg/dL, LDH 209 U/L, normal blood count, normal kidney and liver function. After hospital admission, the patient developed an episode of massive hemoptysis (approximately 650 mL) that required orotracheal intubation, mechanical ventilation, and admission to the ICU. Bronchoscopy, chest X-ray (Figure 1A) and thoracic CT (Figure 1B) findings excluded an active hemorrhage and confirmed the presence of a consolidation in the apicoposterior segment of the upper lobe of the left lung with the air crescent sign. Two major diagnostic hypotheses were formed: pulmonary tuberculosis and aspergilloma. Sputum examination identified acid-fast bacilli (Figure 1C) but not Aspergillus, and the nucleic acid amplification tests detected Mycobacterium tuberculosis. Other laboratory findings of Aspergillus, particularly IgE and IgG antibody, were also negative which did not support the diagnosis of aspergilloma. The diagnosis of tuberculosis was established, and the drug susceptibility testing confirmed the strain was susceptible to therapy with isoniazid, rifampin, pyrazinamide and ethambutol. The follow-up thoracic CT (Figure 1D) after 9 months of treatment, did not show active disease.
Fig. 1
(A) Chest X-ray (posteroanterior [PA]): Consolidation (73×54mm) on the upper third of the left lung; (B) Chest CT (axial plan [AP]): Consolidation in the apicoposterior segment of the upper lobe of the left lung with a central cavitation and the air crescent sign; (C) Acid Fast Bacilli from sputum examination, Ziehl-Neelsen; (D) Chest CT (axial plan [AP]): Nodular and sub nodular images, probably sequelae in the posterior segment of the left upper lobe, with some distortion of the bronchovascular architecture and associated pleural thickening
Tuberculosis and aspergilloma can both cause life-threatening hemoptysis1 when complicated by cavitation. Although the air crescent sign is a characteristic imaging finding of aspergilloma, it can be found in other entities including tuberculosis2, neoplasms (particularly bronchial carcinoma), Rasmussen’s aneurysm, and intracavitary clots. Other, rarer causes include foreign bodies, thick pus, dehydrated caseous material, teratoma, and hydatid disease3,4.