

INTRODUCTION
By mid April to early May 2020, as the first pandemic wave was declining in Greece, hundreds of hospitalized patients were discharged with instructions to remain in home isolation1. The restriction of physical activity following a hospitalization is inevitable, with obvious effects on both physical and emotional health2,3. Even healthy adults who have been infected, experience the devastating effects of bed rest and isolation, regardless of hospital stay length4. The phenomenon is more pronounced in patients with chronic underlying diseases, such as chronic respiratory, cardiac and vascular diseases, hypertension, diabetes, and cancer, or obese adults who require additional care to recover to their prior physical ability status5. There is a growing concern about the potential long-term consequences of COVID-19 in hospitalized patients (with or without comorbidities) and in those returning home6. Medical care after hospital discharge should include evaluation of any rehabilitative needs and prioritizing effective and comprehensive interventions, in order to improve patients’ physical, functional, and psychological status6. As tele-rehabilitation provides effective clinical services from a distance, it could be an appropriate intervention at the post-acute period, in order to achieve basic gains in physical capacity, symptoms and quality of life in patients with SARS-CoV-2 infection7. In this context, we aimed to deliver a short-term home-exercise program through tele-rehabilitation sessions for previously hospitalized COVID-19 patients who remained at home isolation during the first lockdown in Greece, emphasizing on patients’ recruitment and retention into the study.
METHODS
Participants
This prospective study recruited patients hospitalized at two referral hospitals, the General Hospital of Athens ‘Evangelismos’ and the University Hospital of Ioannina. Inclusion criteria were: aged 20–65 years, duration of hospitalization longer than 7 days, moderate disease8 during hospitalization and fatigue as the main symptom at hospital discharge. Patients were excluded from the study if they were admitted in the intensive care unit and/or they were advised to use oxygen at discharge. Additionally, patients who had severe cardiovascular, neuromuscular, orthopedic or renal disease, or any hearing, speaking, cognitive impairments and/or serious mental illness or could not communicate adequately in Greek, were excluded from the study8. All participants were maintained through optimal medication if needed due to comorbidities (e.g. diabetes, hypertension, thyroid disease). They were fully informed about the aims of the study and provided a written informed consent sent via email. The study complies with the Declaration of Helsinki and the protocol was approved by both Scientific and Ethics Committees of Evangelismos Hospital (Protocol ID-160/2020) and University Hospital of Ioannina (Protocol ID-356/2020) as well as by the Ethics Committee of the Physiotherapy Department of the University of Thessaly (Protocol ID-336/2020). The study duration was 4 months, from April to July 2020.
Study design
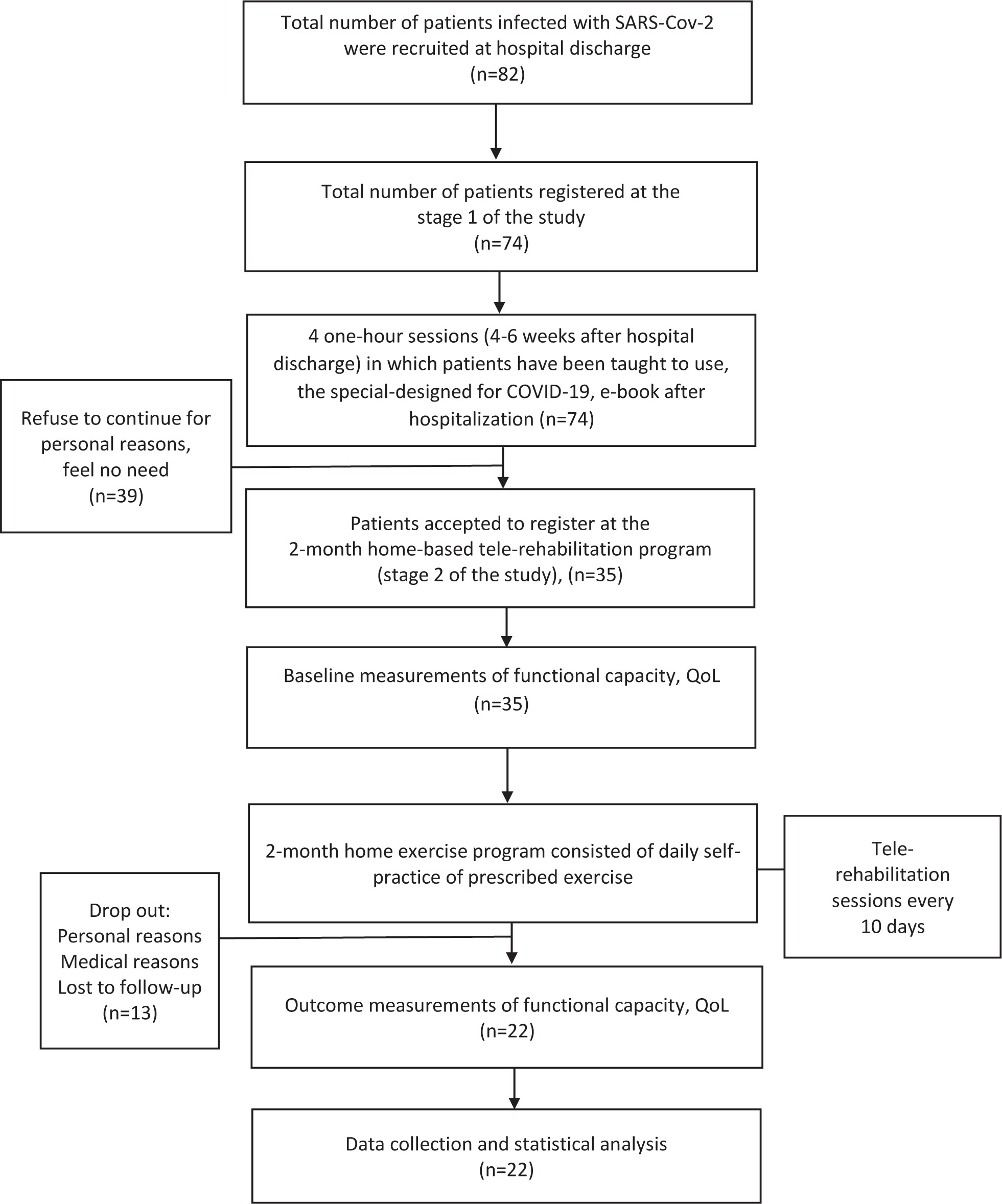
A smartphone app (Viber) was used to establish a two-way tele-communication between physiotherapists and home-isolated patients following hospital discharge. The application enabled interviewing and monitoring patients from the beginning of the study and during all tele-rehabilitation sessions. The study consisted of two stages (Figure 1). During four 1-hour teleconference sessions in the first stage, patients were taught to use a specially designed e-book for patients with COVID-19 and they were asked about their physical and emotional status, their nutritional habits and quality of life after hospitalization. Before entering the second stage, they were assessed via tele-monitoring using three functional tests. During the following 2-month period, the participants continued a home-exercise program consisting of daily unsupervised self-practice of prescribed exercise and a 1-hour individualized and supervised exercise tele-rehabilitation session with a physiotherapist, every 10 days (3 sessions per month). The study protocol was part of a multicenter randomized control trial study which had been registered on Clinical Trial database (NCT04368845).
Physiotherapists’ background
All physiotherapists had more than two years of clinical experience in pulmonary rehabilitation. Before their participation in this study, they had one week intense training regarding remote assessment procedures and tele-rehabilitation approach. Each individual patient was assessed and supervised by one well-trained in remote intervention physiotherapist.
A specific to COVID-19 e-book
As safety and efficacy data on rehabilitation and especially on tele-rehabilitation in patients with COVID-19 are lacking, authors paid attention to a specially designed e-book (https://cutt.ly/AUHcbVw). The e-book included breathing exercises, relaxation, aerobic and total body strengthening exercises along with dietician instructions. Safety instructions and emergency contact details were also included at the end of the e-book. Each part of the e-book was taught to the patients by physiotherapists and a dietitian during the first stage of the study. Ensuring patients’ safety, special attention was given for understanding of all the written information in the e-book, especially those for breathing control during body exercises. More specifically, using the e-book, they were taught to control exercise intensity and to recognize any signs and symptoms of physical distress. They were also instructed how to measure blood pressure, heart rate and oxygen saturation with their own electronic sphygmomanometer and oximeter, respectively.
Daily self-practice of unsupervised exercise
The patients who accepted to continue to the second stage were advised to set 30 minutes per exercise session, 5 times per week. The intensity of exercise training in each session was determined by using the Borg scale 6–20 and it was set at low to moderate level (Borg 9–13) for all participants (Table 1). Some of them gave more attention to upper and lower limb muscle strengthening and others to aerobic training, depending on their individual needs, interest and abilities. Each exercise session consisted of a 5–10 min warm-up session of breathing exercises combined with dynamic movements exercises (e.g. arm rotations, chest expansions) and balance training (one-leg stands, tandem stands, and tandem walking). The main workout consisted of 15–20 min of lower limb strengthening exercises and weight bearing training. Individualized strengthening exercises for upper and lower limbs were carried out in a progressive sequence from the seated position to the standing position using dumbbells, ankle weights and elastic bands. Strengthening exercises started with 0.5 kg weight and progressed by applying additional weight (0.5 kg every week up to 1.5 kg). Participants were initially instructed to complete up to one set of 8–12 repetitions for each type of exercise (e.g. arm abduction, flexion, rotation; elbow flexion, extension; hip abduction, flexion, rotation; knee extension; body weight exercises for upper and lower limbs; body weight squats), which gradually increased even to 15–20, so that the training load would produce muscle fatigue up to 12–13 (somewhat hard) on Borg 6–20 scale. At the end of the main workout, all participants did 5–10 minutes of cool-down exercises focused on slow movements and stretching of the upper and lower limbs, allowing the heart rate to return back to normal values and to improve flexibility. During each exercise session, heart rate and arterial oxygen saturation (SpO2) were monitored continuously by pulse oximeter placed on the right middle finger9. Additionally, patients were prompted to focus and correct their breathing pattern in order to avoid hyperinflation while exercising10. Before and after each exercise session they had to measure and to report their blood pressure, heart rate and oxygen saturation. Both Borg scales 0–10 and 6–20 were used by patients to evaluate any dyspnea (breath discomfort) or fatigue (body discomfort), respectively. The use of both Borg scales was decided by the physiotherapy team in order to avoid false reporting by the patients and misinterpretation. At the end of each exercise session, all reports (heart rate, SpO2, fatigue and dyspnea) were sent by patients or by their caregivers, via Google Forms to an electronic database in order to monitor adherence and exercise safety. Patients were asked to stop exercising and call the team coordinator (EK) if any signs of physical distress such as muscle weakness, shortness of breath, chest pain were observed. Additionally, the team coordinator checked daily the patient electronic database to detect any adverse sign during exercise sessions. During the individualized tele-rehabilitation session, the exercise training was supervised by a physiotherapist and new goals were set (e.g. adjust training intensity, training time) in collaboration with each individual. Furthermore, the physiotherapist confirmed that all exercise reports had been successfully submitted during the last 10 days.
Table 1
Home-based exercise program of the post COVID-19 patients
Measurements at the 1st Stage
Following 2 to 8 weeks after hospital discharge patients participated in four 1-hour teleconference sessions to provide all the demographics and medical history data. Additionally, they were asked about their physical activity status, anxiety, depression, dyspnea during activities and quality of life after COVID-hospitalization, using the International Physical Activity Questionnaire (IPAQ-Gr)11, the Hospital Anxiety and Depression Scale (HADS)12, the modified Medical Research Scale for dyspnea (mMRC)13 and the Short Form-36 generic questionnaire (SF-36)14, respectively.
Physical activity
IPAQ-Gr includes 7 questions about frequency, duration and intensity of participation in physical activities over the previous 7-day period and used to generate a total physical activity score, expressed in metabolic equivalent (MET-min/week)11. The mMRC scale is a five-category scale to characterize the level of dyspnea during physical activity. The higher scores reflect increased level of dyspnea13.
Health-related quality of life
The Short-Form 36 acute form questionnaire was used. It consists of 36 questions divided into eight subscales of physical and mental health concepts: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. The scores of each subscale range from 0 to 100 with higher scores indicating better physical and mental status. Two overall scales are derived from these eight subscales, one for total physical function (SF-36pcs) and one for total mental function (SF-36mcs)14.
Anxiety and depression
The HADS measures generalized symptoms of anxiety and depression in medically ill patients aged 16–65 years12. Each dimension has 7 items and responses are rated on a 4-point Likert scale ranging from 0 to 3. Total score for each dimension can range from 0 to 21. The higher the score the more severe is the anxiety/depression. The following interpretation of scores is recommended: 0–7 normal or no anxiety/depression; 8–10 mild; 11–12 moderate; 14–21 severe anxiety/depression. The mean optimal cut-off score is approximately 8 plus in each dimension resulting mean sensitivity and specificity at 80% and at 90% for detecting anxiety and/or depression disorders in a community cohort15.
Measurements at the 2nd Stage
All patients were assessed in two separate sessions, one at the baseline of the second stage and another at the end of the 2-month exercise program, via teleconference using the Short Physical Performance Battery (SPPB)16, the 60 sec sit to stand test (60secSTS)17 and the 3-min step test (3MST)18. Written information and a demonstration video were given for each test procedure so as to keep patients well prepared and aware. Patients’ measurements were monitored using the smartphone Viber App by the same physiotherapist. The SPPB was performed initially, followed by the 60secSTS and the 3MST, 30 minutes later. For safety and convenience concerns, a third person (caregiver or partner) witnessed tele-monitoring. Patients were continuously monitored by an oximeter during all tests.
Short Physical Performance Battery (SPPB)
It consists of three timed sub-tests: standing balance test, 4-meter self-paced gait speed (4mGS) and 5-repetition sit-to-stand (5STS). Each sub-test scores from 1–4 units, so the overall SPPB score ranges from 4–12 units. All participants performed the SPPB as described previously16.
The 60 sec Sit-to-stand test (60secSTS)
The test was performed using a chair (45 or 46 cm height, without arm rests). Participants were asked to fold their arms across their shoulders and start to stand up and sit down completely for one minute without any support, as many times as possible and at their own pace17. No encouragement was given during the test and the number of completed repetitions was recorded.
The 3-min Step Test (3MST)
The 3MST was performed on a stair tread (17–20 cm height) at home stairs. If necessary, participants were authorized to put their hand on the wall in case of imbalance. The test started from the standing position; the patients had to step up and down the stair tread with a rhythm of 96 beats per min (24 steps per min), given by a metronome, for 3 min continuously18. The following parameters were recorded throughout the test by a pulse oximeter: oxygen saturation (SpO2) and heart rate. Dyspnea (Borg scale 0–10) and leg fatigue (Borg 6–20) were recorded at the beginning and at the end of the test.
Statistical analysis
Categorical variables were expressed as frequencies and percentages. All variables were tested for normality using the Shapiro-Wilk test. Normal distributed variables are presented as mean and standard deviation (mean ± SD) and not normally distributed variables as median and IQR (25th–75th percentile). Two-tailed paired t-tests were used for within-period comparisons for normal distributed variables, otherwise comparisons were performed by using the Wilcoxon matched-pair test. Differences between independent groups (patients who completed the second stage versus those who dropped out) were tested with independent samples t-tests or Mann Whitney test, where appropriate. All statistical analyses were performed using SPSS for Windows 22.0 (SPSS Inc, Chicago, IL, USA). The level of statistical significance was set a priori at p<0.05.
RESULTS
Results from the 1st Stage
Eighty-two (61 males) clinically stable patients hospitalized for SARS-CoV-2 were recruited from mid April to early June 2020. Of these, 74 (90.2%) clinically stable individuals met all the inclusion criteria and participated at the initial four teleconference sessions, following a median 32 (IQR: 22–40) days from hospital discharge. They presented slight to moderate functional limitations at hospital discharge (Post-Covid-19 Functional Scale, PCFS grade 2 to 3)19. A total of 33 participants (44.6%) were ex-smokers (mean pack-years: 18.6 ± 11.4); 6 participants (8.1%) were current smokers (mean pack-years: 16.3 ± 11.1). Patients’ characteristics, comorbidities and their habits for technology use are presented in Table 2. Most of the participants, 31 (41.9%), were overweight (25< BMI <29.9 kg/m2); 26 (35.1%) obese (BMI >30 kg/m2) and 17 (22.9%) had normal weight (BMI <24.9 kg/m2). Duration of hospitalization ranged 9–17 days, with a mean 13.1 ± 2.9 days.
Table 2
Characteristics, comorbidities and habits of technology use in patients with COVID-19 included at the first stage of the study (N=74)
Results from the 2nd Stage
Thirty-five (47.3%) patients accepted to participate at the second stage of the study. Those who dropped out (n=39) had better physical function after COVID-19 hospitalization, median SF-36pcs score 40.56 (IQR: 37.42–53.79) versus 39.15 (IQR: 27.96–44.33) (p=0.025); were heavier smokers, mean 21.77 ± 11.3 versus 10.4 ± 5.8 pack-years (p<0.001); with lower BMI, mean 27.54 ± 5.5 versus 29.81 ± 2.4 kg/m2 (p=0.022) than those (n=35) who accepted to continue at the second stage. Twenty-two (29.7%) (18 males) completed the 2-month exercise program. Thirteen patients stopped participation 22.6 ± 2.3 days after initiation of the program either for personal reasons (family obligations, lack of personal time, etc.) or for medical reasons (n=1) (scheduled surgical procedures) (Figure 1). The mean age of the participants (n=22) at the second stage was 50.1 ± 13.2 years and the mean BMI was 29.8 ± 2.4 kg/m2. Obesity (54.5%; n=12), dyslipidemia (18.2%; n=4) and hypertension (27.3%; n=6) were the presented comorbidities. The time period elapsed between the onset of COVID-19 infection (positive swab) and the onset of the home-based exercise program (n=22) was 37.1 ± 15.2 days. At the beginning of the intervention the main persistent symptoms were anxiety (n=19; 86.3%), body fatigue (n=16; 72.7%), and cough (n=2; 9.1%). All participants attended in total 6 private tele-rehabilitation sessions with the same physiotherapist. The mean number of self-practice exercise sessions was 18.4 ± 3.5. The training program was well tolerated by all 22 patients and no adverse effects were observed either during initial and follow-up assessment via Viber tele-communication or during home-exercise sessions. There were no dropouts related to symptom worsening. For all exercise sessions, the mean final SpO2 was 95.6% ± 1.4% and the mean final heart rate was 128.2 ± 7.6 pulses per min; 70.9% ± 4.1% of the predicted maximum heart rate. Most of the participants (n=20) followed a strengthening exercise program for both upper and lower limbs and only 2 participants combined strengthening and aerobic (in-home cycling) exercise. At baseline and after the program completion, all physical capacity and psychological results are presented in Table 3 and Table 4, respectively.
Table 3
Functional capacity at baseline and after the 2-month exercise program in patients with COVID-19 (N=22)
| Variable | Pre Intervention Median (Q1–Q3) * | Post Intervention Median (Q1–Q3) * | p |
|---|---|---|---|
| SPPB total score, units | 9 (8–11) | 10 (8–12) | 0.174 |
| SPPB subtests | |||
| Balance, units | 4 (4–4) | 4 (4–4) | 1.000 |
| 4mGS, units | 2 (2–3) | 3 (2–4) | 0.459 |
| 5STS, units | 3 (2–4) | 3 (2-4) | 0.397 |
| 60secSTS, number of repetitions | 22 (20–25) | 31 (25–36) | <0.001 |
| 3MST | |||
| HR, beats/min (end test) | 101 (92–122) | 101 (92–113) | 0.569 |
| Delta HR | 28 (19–45) | 19.5 (10–34) | 0.852 |
| SpO2 (%) (end test) | 96 (95–97) | 97 (95–98) | 0.180 |
| Delta SpO2 | 0 (-3–0) | 0 (0–1) | 0.120 |
| Dyspnea (end test), Borg (0–10) | 1.5 (0–4) | 1 (0–2) | 0.957 |
| Lower limb fatigue (end test), Borg (6–20) | 7.5 (7–13) | 7 (6–9) | 0.050 |
SPPB: Short Physical Performance Battery. 4mGS: four-meter gait speed. 5STS: five sit-to-stand. 60secSTS: 60 second sit-to-stand test. 3MST: 3-Minute Step Test. HR: heart rate. Delta HR: HR end of the test - HR start of the test. SpO2: pulsed oximetry. Delta SpO2: SpO2 end of the test - SpO2 start of the test.
Table 4
The level of physical activity, quality of life, anxiety, depression, mMRC at baseline and after the two-month exercise program in patients with COVID-19 (N=22)
| Variable | Pre Intervention Median (Q1–Q3) * | Post Intervention Median (Q1–Q3) * | p |
|---|---|---|---|
| IPAQ-Gr | |||
| Total score, METs-min/week | 693 (80–1314) | 825 (422–2220) | 0.131 |
| SF–36 | |||
| Physical Component Summary, units Mean ± SD | 37.5 ± 10.3 | 52.1 ± 6.0 | <0.001 |
| Mental Component Summary, units Mean ± SD | 42.9 ± 11.6 | 45.5 ± 12.3 | <0.001 |
| Physical functioning, units | 40.2 (29.9–48.6) | 52.7 (50.7–54.7) | <0.001 |
| Role physical, units | 27.4 (20.1–56.8) | 54.5 (35.7–54.5) | 0.001 |
| Bodily pain, units | 45.2 (24.5–57.9) | 53.1 (35.2–55.5) | 0.235 |
| General health, units | 44.8 (38.6–48.1) | 50.1 (47.6–57.5) | 0.008 |
| Vitality, units Mean ± SD | 42.7 ± 11.6 | 48.8 ± 11.1 | 0.006 |
| Social functioning, units | 35.0 (24.1–40.4) | 57.9 (52.4–57.9) | <0.001 |
| Role emotional, units | 48.1 (32.5–55.8) | 56.9 (33.2–56.9) | 0.175 |
| Mental health, units | 44.3 (33.1–52.8) | 51.0 (22.2–53.8) | 0.638 |
| HADS | |||
| HADS anxiety score, units | 9.0 (6.0–13.0) | 4.3 (3.2–9.6) | 0.006 |
| HADS depression score, units | 5.0 (3.0–8.0) | 1.8 (0.9–3.7) | 0.001 |
| mMRC score, units | 1.0 (0–1.0) | 0 (0–0.9) | 0.001 |
DISCUSSION
This single-cohort interventional study demonstrated that a 2-month home-based rehabilitation program combined with regular tele-rehabilitation sessions, for home-isolated post-COVID-19 patients with slight to moderate functional limitation, was safe, feasible and effective for improving anxiety, depression, quality of life as well as lower extremity physical performance after hospitalization (Tables 3 and 4). Early in 2020, there were studies reporting that COVID-19 patients had reduced levels of physical function, muscle weakness and fatigue, as well as impaired psychological health and poor quality of life20-22. More recent studies have shown that these consequences were evident even at 6 months post hospitalization23. To date, very few randomized controlled trials have demonstrated a slight improvement in physical function (as it was assessed using either the 6MWT or the 60secSTS) and in QoL within the first short-term rehabilitation period (3–6 weeks) following hospitalization21,24,25. Two of these RCTs used unsupervised tele-rehabilitation approaches lasting one or six weeks (3–4 sessions per week)24,25. For patients’ reinforcement and exercise feedback, the home-based exercise program was monitored every week via videoconferences by physiotherapists. All the functional outcomes (6MWT, sit-to-stand tests) and QoL have been improved after intervention; however, none of them has been assessed remotely, using smartphone applications. Adding to previous research, in this study we used an 8-week tele-rehabilitation approach which included remote functional assessment and we found a partial recovery in physical performance with no adverse event or symptom worsening. During this period, there were strict lockdown measures in Greece in combination with the successful prevention of the health system oversaturation1. In this 3-month timeframe all state or private rehabilitation programs were cancelled to prevent disease spread. Nevertheless, our intervention was well-designed in order to provide immediate and prompt care in patients with physical and psychological impairment who remained in isolation after hospitalization. With the assistance of technology, our remote intervention achieved the desired result and the adherence to program implementation was satisfactory (patients completed a mean of 18 exercise sessions). Personal reasons and lack of time for regular exercise were reported only from those who dropped out (n=13) after three weeks of participation.
The study of Belli et al.22 in a large cohort of patients (n=103) showed that after 3 weeks of mobilization, physical function was not improved in all patients. The SPPB score was still low (0–6 units) to moderate (7–9 units) in 70.8% of the patients, and 33.3% of the patients noticed 60secSTS repetitions less than the normal reference values17. In our study, the baseline SPPB score was moderate, indicating a population with a low risk of disability16 and it was slightly but not significantly (p=0.174) increased to high performance score (10–12 units) after the 2-month rehabilitation program, indicating full recovery. Although the number of repetitions in the 60secSTS improved significantly after the rehabilitation program and also exceeded the minimal clinical importance difference (2.5 repetitions), previously reported for patients with chronic respiratory diseases26, it was still lower (Table 3) than the normal reference values (median > 34 and 37 repetitions for healthy women and men aged up to 64 years, respectively)17.
Published research findings showed that the 6MWT was the main outcome measure for testing physical function in patients with COVID-1920,21. However, knowing that the 6-minute walking distance cannot be accurately assessed at home in patients with chronic respiratory disease27, the 3 min step test was used in our cohort of COVID-19 patients as an alternative test to assess cardiovascular and respiratory fitness. Both 60secSTS test and 3MST are correlated to 6MWT in healthy young people28 and in patients with COPD29. To the best of our knowledge, no previous studies used 3MST for assessing cardiorespiratory fitness in post COVID-19 patients, although more rigorous step tests had been used in the past in patients recovering from SARS30. In our study, no adverse effects or desaturation were observed during the test and improvement was reported only on leg fatigue. To validate these findings, further research is needed to determine whether 3MST can accurately assess functional capacity when used remotely.
Finally, health-related quality of life as well as anxiety and depression improved over the 2-month period (Table 4), however, we cannot deduce that this was due to the exercise program due to the absence of a control group. The scores are somehow lower than in healthy individuals31 and similar to those previously presented in studies with long-term outcomes (up to 6 months after hospitalization) from other coronavirus infections (SARS, MERS)30,32.
During the study we faced barriers to the remote physical assessment and to the delivery of the exercise program. During the remote assessment, one of the barriers could be providing comprehensive guidance to both the patients, when performing the functional tests, and the third person (caregiver or partner) who witnessed the tele-monitoring (for observing any adverse effects, e.g. high blood pressure, excess breath discomfort, high heart rate, etc.). Another barrier could be the short-time of the intense training that each physiotherapist had to complete, in order to be able to deliver the functional assessment by distance and to supervise exercise program. To overcome some of the above barriers, we took actions to facilitate our intervention. Written instructions and videos were given to the patients; four 1-hour sessions included at the first stage of the study, in which all participants were taught how to perform exercises at home and to control exercise intensity; direct uploading of the results of each session to an electronic database via Google Forms facilitated patients’ understanding on exercise prescription and enabled the rehabilitation team to monitor program adherence and any exercise adverse effects. We propose that future tele-rehabilitation should also assess the validity of commonly used functional tests when they are performed remotely, as well as the competency of the healthcare professionals in remote assessment and clinical practice. We recognize that this was not a formal comprehensive interdisciplinary rehabilitation program as was previously described in chronic respiratory patients33. However, early April 2020, it was proposed that rehabilitation programs can be conducted remotely by healthcare professionals in isolated COVID-19 patients34. Later on, the feasibility and the potential of success of telehealth physical therapy implementations has been provided35 and we think that the present study adds further to this field.
Limitations
The study has several limitations, mainly owing to the nature of the assessment environment and the absence of a control group. Due to isolation restrictions, all assessments were made through tele-conferences. Therefore, we cannot rule out experimenter bias or guarantee reliability of the functional tests in domestic environment. Important factors should be taken into consideration when evaluating outcomes of remote assessment conditions and we point out that further research is needed in this field. The single-group experimental design is not able to establish whether the intervention led to the changes in these specific outcomes. Nevertheless, this design has been adopted from other studies which tried to deliver early rehabilitation services in post-COVID-19 patients (n=30)36 following the first published recommendations of European Respiratory Society and American Thoracic Society6. Of course, more randomized control trials, exploring rehabilitation outcomes in patients with COVID-19 who participate in remote exercise interventions, may provide further information, with acknowledgement of the results of both this study and previous observational single-cohort studies36.
An additional limitation was the small number of participants who completed the second stage of the study, maybe due to the loss of human contact (face-to-face interaction) with physical therapists, the sparse tele-rehabilitation sessions (every 10 days) or even patients’ perceptions of their real needs. For example, many patients declined to participate in this study as they felt they had other health and/or personal issues to face. Nevertheless, for patients who completed, adherence to the exercise program (completing in total 24–28 exercise sessions in 2 months) was comparable to that previously reported in the outpatient pulmonary rehabilitation setting33.
Finally, this study included only patients aged 18–65 years, hospitalized at medical wards. Up to 30 June 2020, the National Public Health Organization in Greece reported 2328 cases of COVID-19 in patients up to this age. The choice of this age group was made to diminish any limitations to technology access and provide services to the age group that is most often hospitalized37. Therefore, this approach may limit the generalizability of these findings to all the spectrum of the severity of COVID-19 disease and patients’ age.
CONCLUSIONS
A two-month personalized, unsupervised, home-based exercise program combined with tele-rehabilitation sessions was safe, feasible and it partially improved the impaired physical performance and psychological status in COVID-19 patients after hospitalization. There was positive adherence to the tele-rehabilitation program and these findings encourage implementation of telehealth for the long-term management of post-COVID-19 patients’ physical and psychological health.